A 59 year old female with CAP
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comments
A 59 year old female, homemaker by occupation, came to the causality with c/o fever since 6 days, cough since 5 days, SOB since 2 days, pain abdomen since afternoon
History of presenting illness:
Patient was apparently asymptomatic 6 days back. Then she developed fever which was high grade, associated with chills.
Fever subsided now.
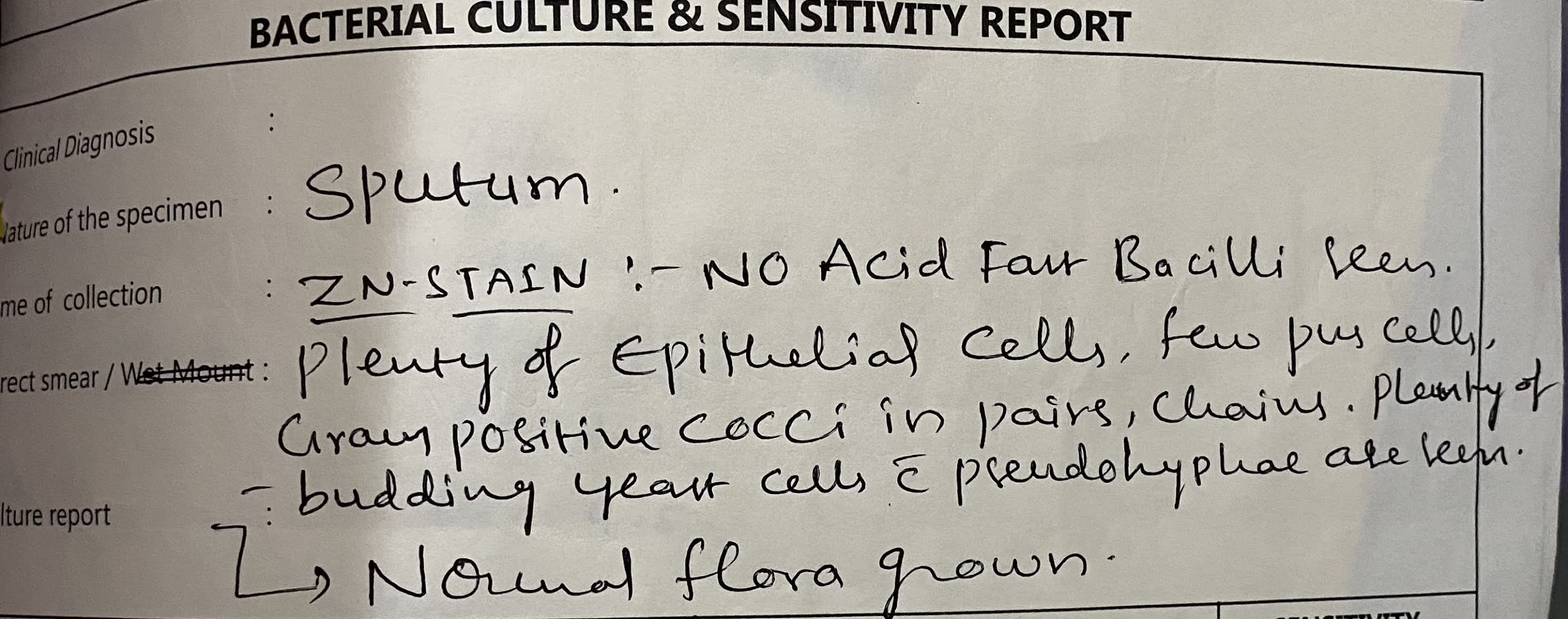
-Cough with sputum , blood tinged since 5 days
- chest pain since 5 days
-Grade 4 Shortness of breath since 2 days
-No H/o vomitings, diarrhea
-No h/o palpitations.
-She was diagnosed with DM last year and is on ayurvedic medication for it.
- k/c/o CKD ?
Past history:
K/c/o DM on medication
K/c/o ckd?
Personal history:
Mixed diet
Appetite normal
Micturition normal
Bowels normal
No addictions
Family history:
Not significant
General examination:
Patient is c/c/c
Moderately built and nourished
Pallor present
No icterus, cyanosis, clubbing, koilonychia, lymphadenopathy, edema
Vitals:
Temp- afebrile
BP- 130/80 mm hg
PR -120 bpm
RR- 56/min
SpO2 - 93% at room air
GRBS - 241 mg/dl
Systemic examination:
CVS: s1s2 heard
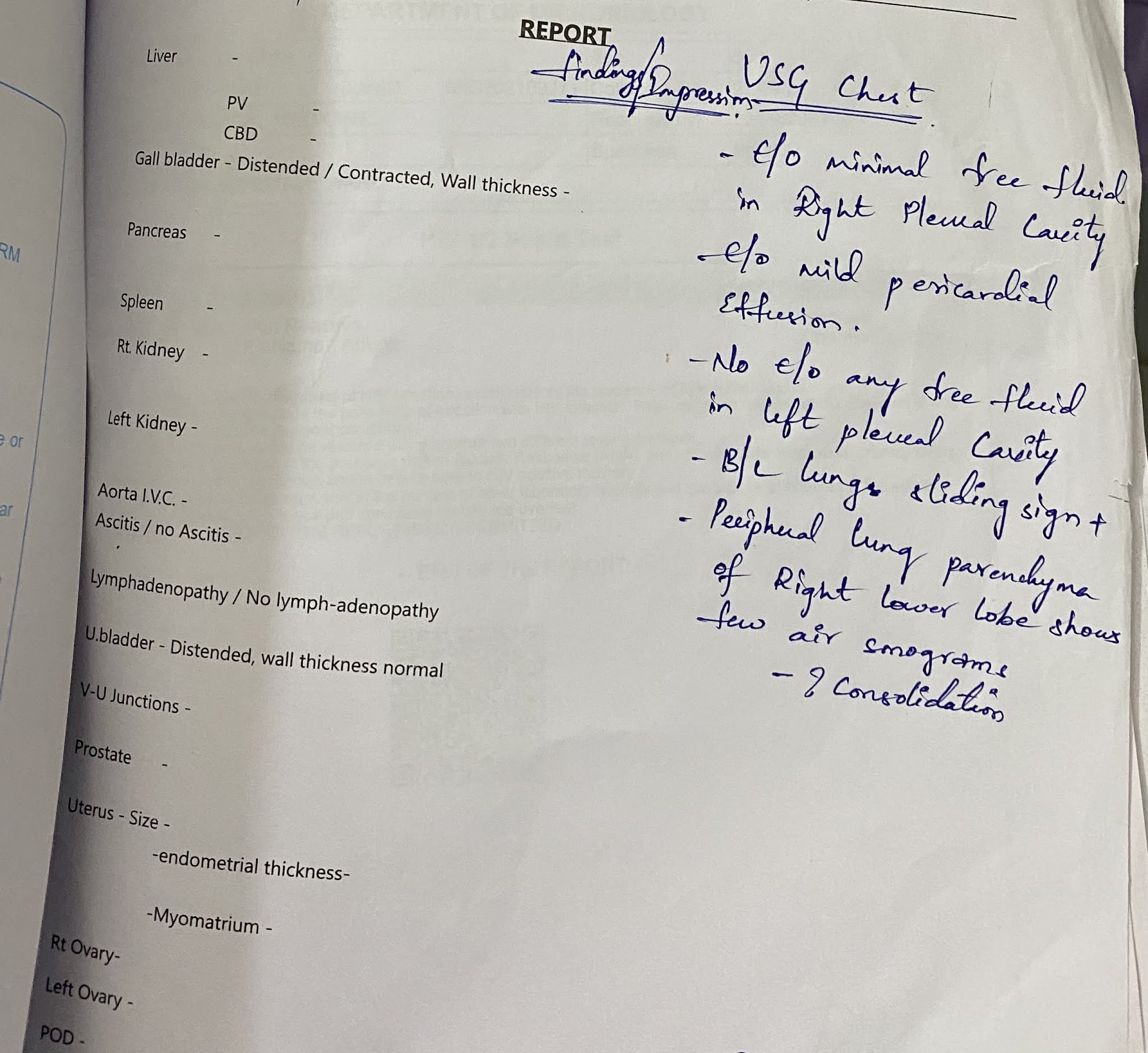
RS: BAE + B/L coarse crests heard in R>>L
P/A: soft, non tender, BS+
CNS: NFND
Investigations:
Serum creatinine- 4.9mg/dl
Blood urea - 177 mg/dl
ALP- 234 IU/L
X ray: abdomen:










Provisional diagnosis:
Community acquired pneumonia
With k/c/o DM
With k/c/o HTN??
With AKI on CKD with sepsis
? Pyelonephritis
Treatment:
- Inj. Meropenem 1g/IV/STAT f/b 500 mg IV/BD
- Inj pan 40 mg IV/OD
- IVF: NS and RL @50ml/hr
- Inj OPTINEURON 1 ampoules in 100 ml NS IV/OD
- Temp charting 4th hrly & tepid sponging
- Nebulisation with Duolin and bud escort 8th hourly
- O2 inhalation
- GRBS charting 6th hourly
- Inj HAI s/c/TID
- Strict I/o charting
- Monitor BP, PR, RR

















Comments
Post a Comment